Stebbins, Cocohoba leading specialty drug study with Walgreens

So-called specialty drugs can represent lifesaving advances in the treatment of serious complex conditions, such as cancers, hepatitis C, rheumatoid arthritis, multiple sclerosis, and inflammatory bowel disease. They can turn once routinely lethal diseases such as HIV and cystic fibrosis into manageable chronic conditions. They can address rare genetic conditions, such as hemophilia, or suppress immune rejection after organ transplants.
But getting these drugs to the patients who need them—addressing issues of access and affordability that interfere with their ability to take them as prescribed (adherence)—has presented ongoing challenges.
Barriers to specialty drug adherence
UCSF School of Pharmacy faculty members Marilyn Stebbins, PharmD, and Jennifer Cocohoba, PharmD, recently entered into a $646,000 contract with Walgreens, the largest drug store chain in the U.S., to more fully and precisely determine those impediments. The goal is to gather evidence that may provide the basis for new, more effective models of specialty pharmacy care.
The study will gather and integrate the perspectives of patients, health care providers, specialty pharmacists, and their staffs, via interviews and focus groups. While open-ended in its approach, the study will evaluate the importance of hypothesized impediments that include:
Out-of-pocket costs
Specialty drugs are expensive: see Facts and figures: costs and benefits of specialty drugs. In fact, insurance plans define these medications by their prices. For example, Medicare’s Part D drug benefit defines specialty drugs as costing $600 or more a month, and many cost considerably more. Typically, they require a coinsurance payment that can be a percentage of that hefty drug price.
There are often co-pay assistance programs to help patients who qualify, but these require additional steps and knowledge by patient and providers.
Prior authorization hurdles, disease-related testing requirements
Costliness may mean that a specialty drug is only covered by insurance when less expensive options are inappropriate for a condition or have been found ineffective. In addition, a specialty drug may be targeted for a particular subtype of a condition, so additional testing may be necessary.
Both cases require additional documentation, sign-offs, and time—which can interfere with starting or continuing a prescribed drug regimen.
The system is disconnected and confusing, such that it actually may serve as its own barrier to patients taking these medicines.
—Jennifer Cocohoba, PharmD
Disease expertise, counseling needs, self-administration of drugs
Specialty drugs often need to be injected (sometimes by the patients themselves) or infused (given intravenously) and they can require special handling, such as temperature control. So there is a need for ongoing counseling to monitor and manage side effects, run follow-up tests, and ensure patients are taking the drugs properly.
The study will help evaluate if there is a need for 24-hour support services for some specialty drugs.
Specialty pharmacies seek to address challenges
To address those challenges, pharmacy chains (including Walgreens) have established specialty pharmacies that contract with insurers and only handle prescriptions for these drugs. Most are mail-order operations, in which pharmacists expert in particular drugs and conditions interact with prescribers and patients by phone and via electronic prescriptions.
Centralization of expertise and inventory—Walgreens, for example, has four centralized specialty pharmacies covering the entire country—can make logistical sense, given that conditions treated by specialty drugs are relatively rare. So, centralized mail-order pharmacies help to ensure patient access to the expertise of specialty pharmacists and drugs, without long-distance travel. In addition, expensive medications don’t reach their expiration dates sitting on the shelves of general retail pharmacies.
But as Stebbins and Cocohoba point out in a recent interview, this new realm of specialty drug distribution has created challenges of its own.

Q&A with Jennifer Cocohoba and Marilyn Stebbins
Marilyn Stebbins and Jennifer Cocohoba are faculty members in the Department of Clinical Pharmacy, as well as practicing clinicians with extensive experience dealing with specialty medications.
Stebbins serves as the department’s vice chair of clinical innovation and spent 17 years leading a PRICE Clinic (Pharmacist Review to Increase Cost Effectiveness). The clinic, along with providing comprehensive medication management, assists patients in decreasing their out-of-pocket drug expenses while accessing needed medications.
Cocohoba has practiced for 12 years with the Women’s HIV Program at UCSF. Essentially all HIV drugs are specialty medications, she notes, due to both their high prices and the need for clinical expertise to monitor side effects and potential interactions, since the drugs are routinely given in combination.
Jacobson: While understanding that your study design is open-ended, since specialty drugs are routinely defined by high price, how do you see co-payments and higher out-of-pocket costs affecting patient adherence?
Stebbins: The patient walks into the pharmacy, where they’re told: “That’ll be $600.” Or $3,000. And the patient says, “I’ll pick it up tomorrow.” And they never come back, because nobody’s talked to them about the cost issue.
To them, that isn’t coinsurance. People are used to $50 for a brand new drug. That makes it sound like the insurance isn’t covering anything, right? But it’s really typically a 30 percent co-payment in most instances.
Oncology is a very good example. You start someone on a chemo regimen and they get their first bill and they stop it. The worst thing you can do is get them to start it, spend a lot of money, and then stop it. There are clinical [effectiveness] implications. It doesn’t do any good to get that person on a medication if they’re not going to adhere.
Jacobson: Why aren’t they told by their prescriber how much it will cost, so the issue can be dealt with at that point?
Stebbins: Right now, many providers don’t even know the cost of these drugs. So when a provider looks to see whether this is the right therapy for this patient, the system needs to be transparent enough that the provider understands what the patient is going to jump into, from the perspective of cost… and what programs are available to assist the patient—both from a cost and an adherence basis. So it really starts at the prescription.
Cocohoba: I think the fragmentation of the system [with patients getting different drugs from different pharmacies] has made the role delineation even less clear than it was before. Is it the specialty pharmacy’s responsibility to help the patient with co-pay assistance? Is it the doctor’s? How much does the patient have to advocate for themselves? The roles and responsibilities are not clearly defined.

Jacobson: Is such aid to patients part of the specialty pharmacy role? What are real-world challenges to that?
Stebbins: That was the promise of specialty pharmacies—that someone would help you through the process of applying for co-pay assistance, and basically diminishing the cost issue for the patient as best they could. All that could be done over the phone.
The key is: Does the patient get a phone call back? Remember, this often isn’t a walk-in, face-to-face moment. This is a prescription that gets electronically prescribed to a [centralized] specialty pharmacy. How does that pharmacy reach out to a patient? Does the patient answer their phone? There are all these things that can get in the way of that contact happening.
Jacobson: What other real-world complications do you see emerging from this new realm of centralized specialty pharmacies?
Stebbins: There’s a distribution model that’s different for specialty meds than for all their other medications. And the biggest problem is providers don’t understand this, so they don’t know where to send the prescription. Patients don’t understand it, so they take the prescription—or it’s electronically prescribed—to their regular pharmacy, which then says, “We can’t do this.” And they may not know who to direct them to. So there’s this major stop point.
Cocohoba: We’re fragmenting care, making people go to different pharmacies [for different drugs]. You’ve created systems to help manage patients better, in theory. But the system is disconnected and confusing, such that it actually may serve as its own barrier to patients taking these medicines.
Jacobson: Anecdotally, how do you see this confusion playing out in your practice?
Cocohoba: Some private insurance companies require patients to use one mail-order pharmacy for medications you take regularly—like diabetes and high blood pressure medicines—but they require you to use a different mail-order pharmacy for your HIV specialty drugs. A patient may end up using three pharmacies: one located in their neighborhood for picking up short-term prescriptions, one mail-order pharmacy for medications used regularly, and another mail-order pharmacy for specialty medications!
For example, I have a patient who comes to us [UCSF Women’s HIV Program] all the way from the Central Valley to get high-quality care, because there aren’t a lot of HIV specialists there. She was pregnant and doing quite well. She has two other uninfected children because she was taking her HIV medicines during her pregnancies. She was in her last trimester and at that point, because of metabolism changes, we increase the dose of certain HIV medicines to ensure adequate blood levels—in this case, she needed to increase her dose of Reyataz [atazanavir].
Her provider recognized this and called me. She was due in two weeks. I called her local pharmacy and tried to prescribe the medicines, but they were not covered because her insurance mandates that she use a specialty pharmacy. So I called her insurance company and was mistakenly given the number for the mail-order pharmacy—her insurance mandates that she use that pharmacy for any chronic medications. Called them, went through the whole process of trying to submit a prescription and they said, “Oh wait, actually that has to go through the specialty pharmacy. Let me transfer you.”
Luckily, at that point, I did reach a pharmacist who understood the medicines and was able to take the prescription. But here I’m hours on the phone and we need to get her this medicine right away. To their credit, they were able to overnight it to her. But how many steps did it take for me to get through the process?
Stebbins: When a provider sees a patient, it’s insurance agnostic. They don’t even know what the patient’s insurance is, to know what steps and hoops they have to go through.
[Through this study] we want more information so that programs can be designed to address these barriers. How do we get better care to patients requiring specialty meds?
Facts and figures: costs and benefits of specialty drugs
-

Specialty drugs Rx < 1%: fewer than 1% of prescriptions in the U.S. are specialty drugs. 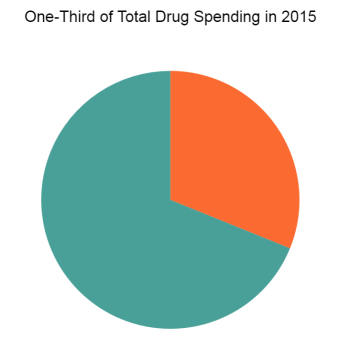
One-third of Total Drug Spending in 2015: Specialty drugs were 1/3 of total drug costs in 2015. While fewer than 1 percent of all U.S. prescriptions are for specialty drugs, in 2015 they represented a third of total drug spending—and that is expected to rise to 50 percent in the next ten years with more such drugs and their wider use, according to IMS Health.
-
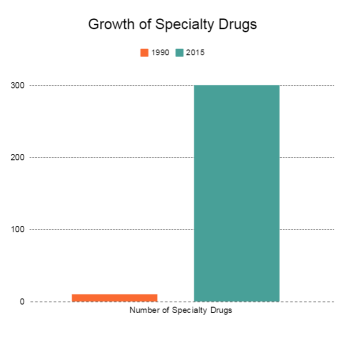
Growth of specialty drugs: the number of specialty drugs grew from 10 in 1990 to 300 in 2015. There were ten specialty drugs on the market in 1990 and nearly 300 in 2015, according to the American Journal of Managed Care.
-
A 2013 study in the Journal of Managed Care Pharmacy found that the cost of specialty drugs for patients treated for chronic conditions (rheumatoid arthritis, multiple sclerosis, psoriasis, inflammatory bowel disease) were more than half of the total cost of care.
-
Patients often face higher out-of-pocket costs for specialty drugs because insurance plans may require a coinsurance payment, a set percentage of a drug price as high as 33 percent, note analyses by the Pew Charitable Trusts and the Kaiser Family Foundation.
-
Specialty drugs like Sovaldi (sofosbuvir) for hepatitis C have made headlines with their cost: about $84,000 for a course of treatment, or $1,000 per daily pill. But the drug can cure more than 90 percent of infected patients in 12 weeks. Thus, while increasing drug spending per se, the medicine can prevent tens of thousands of deaths annually and save money by reducing a patient’s risk of liver cancer, liver failure, and the need for a liver transplant by more than 80 percent.